- Visibility 105 Views
- Downloads 24 Downloads
- DOI 10.18231/j.johs.2024.015
-
CrossMark

Correlation of dermatoglyphics, def index and caries activity test for caries risk assessment in children: A randomised clinical trial
- Author Details:
-
 Manisha Upadhyay *
Manisha Upadhyay *
-
Jyoti Sharma
-
Ankita Agrawal
-
Bhagwat Swaroop Sharma
-
Shashi Prabha Yadav
-
Ankur MIshra
Introduction
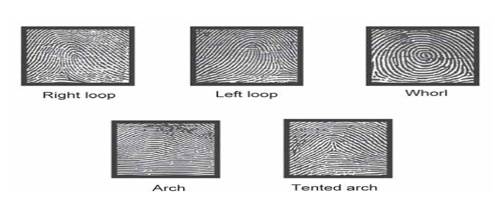
“Dermatoglyphics” is a scientific term used for Palmistry, originated from two greek words “dermo” means skin and “glyphics” means carving.[1] It is study of palmer and planter carvings on hands and feet, these patterns or configurations are genetically determined and remains constant throughout one’s life.[2] ([Figure 1])
The epithelial lining of finger bud as well as that of enamel both has ectodermal origin and both have same time of origin of intrauterine life, i.e., during 6th-13th week of intrauterine life, this is the basis of considering dermatoglyphic pattern as centric marker of dental caries. [3]
Increased count of S. Mutans in saliva/ oral cavity is an indication for high caries risk. The test results can also be used to motivate patients and to determine patient compliance with treatment regimes.[2] Salivary bacterial counts, e.g. Streptococcus Mutans Screening Test (Streptococcus Mutans Adherence Method) are widely used in clinical practice in caries risk assessment. Caries activity tests are based on the concept that S. mutans is the principle causative organism for dental caries.[4]
Regarding the caries index, the ‘def’ index was described by GRUEBBEL A.O. in 1944, as an equivalent index to DMF index, for measuring dental caries in primary dentition. The caries indices used for primary dentition are ‘deft’ index and ‘defs’ index equivalent to the DMFT and DMFS indices used for permanent dentition. As defined by Gruebbel, d = decayed tooth, e = extracted tooth and f = filled tooth. The basic principles and rules for def index are the same as that for DMF index.[5]
Aim and Objective
The present study aims to predict the occurrence of dental caries in children by Dermatoglyphic patterns, Caries activity test and ‘def’ index and to correlate these three methods in caries risk assessment of children.
Materials and Methods
Inclusion criteria
Patients aged between 3-6 years were randomly selected for the study.
Exclusion criteria
Children with special health care needs were excluded.
Dermatoglyphics Pattern Recording and Interpretation
This study was conducted on 300 children coming to the department of pedodontics and preventive dentistry, UCMS, Bhairahawa city, Nepal, after taking ethical clearance from the institutional review committee. Duration of the study was February 2024 to April 2024. An informed consent from the parents was taken before the onset of the study.



‘def’ index recording
The oral examination was done in proper lighting and ‘def’ indices were recorded using diagnostic instruments (mouth mirror, tweezer, explorer). ([Figure 3])
Salivary Bacterial Count Estimation
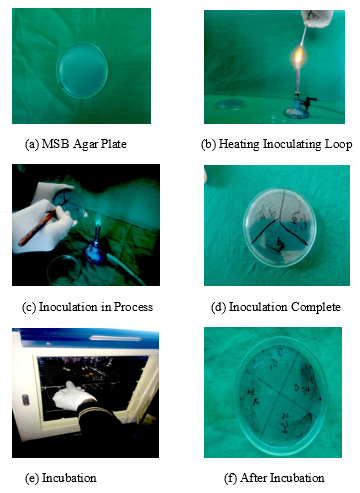
Unstimulated saliva (0.1ml) was inoculated on mitis salivarius bacitracin (MSB) agar. Inoculated plates were set at 600C angle and incubated aerobically at 370C for 24 hrs. After growth has been observed, the supernatant medium is removed and the cells adhering to the glass surface are examined through magnifying glass and scored as follows. [6] ([Figure 5] 5 a-f)
All kinds of morphology of colonies present on each plate were processed for gram staining. The colonies which were blue tear drop type on MSB broth were suggested as S. mutans on gram staining. After recording all the readings, data was sent for statistical analysis.
Result
Data were summarized as Mean ± SE (standard error of the mean). Groups were compared by one factor analysis of variance (ANOVA). Pearson correlation analysis and simple linear regression analysis were done to assess correlation and strength of association between the variables respectively. A two-tailed (α=2) p value less than 0.05 (p<0.05) was considered statistically significant. Analyses were performed on SPSS software (windows version 17.0).
Comparing the mean S. mutans count between different whorl groups, different loop groups and different def index score groups ANOVA showed significantly different S. mutans among the groups (F=170.55, p<0.001), (F=245.82, p<0.001) and (F=93.22, p<0.001) respectively. The association between S. mutans count and number of whorl in children also showed a positive trend suggesting that as number whorl increases, mean S. mutans count also increases. ([Table 1], [Table 2], [Table 3])
The S. mutans count showed a significant and positive (direct) correlation with both whorls (r=0.75, p<0.001) and def index scores (r=0.72, p<0.001) indicating a direct association of S. mutans count with whorls and def index scores. In contrast, S. mutans count showed a significant and negative (inverse) correlation with loops (r=-0.82, p<0.001) indicating an inverse association of S. mutans count with loops.
|
Whorl (no) |
n |
S. mutans count (CFU/ml) (Mean ± SE) |
F Value |
P value |
|
0-2 |
23 |
7.26 ± 0.34 |
170.55 |
<0.001 |
|
2-4 |
49 |
9.29 ± 0.80 |
|
|
|
4-6 |
48 |
35.10 ± 1.17 |
|
|
|
6-8 |
119 |
34.29 ± 0.72 |
|
|
|
8-10 |
61 |
36.08 ± 1.13 |
|
|
|
Loop (no) |
n |
S. Mutans count (CFU/ml) (Mean ± SE) |
F Value |
P value |
|
0-2 |
103 |
37.27 ± 0.85 |
245.82 |
<0.001 |
|
2-4 |
125 |
33.02 ± 0.65 |
|
|
|
6-8 |
60 |
8.87 ± 0.67 |
|
|
|
8-10 |
12 |
7.50 ± 0.49 |
|
|
|
Def index (score) |
n |
S. mutans count (x102 CFU/ml) (Mean ± SE) |
F value |
P Value |
|
0-3 |
78 |
12.62 ± 1.26 |
93.22 |
<0.001 |
|
3-6 |
28 |
35.29 ± 2.37 |
|
|
|
6-9 |
68 |
28.47 ± 0.93 |
|
|
|
9-12 |
84 |
37.55 ± 0.73 |
|
|
|
12-15 |
42 |
36.36 ± 1.24 |
|
|
Discussion
Causation of dental caries in mineralised portions of human teeth has a multifactorial etiology, which can be divided into various subtypes.[7] In the present study two such important parameters have been considered, first one being dermatoglyphics which is genetic component and salivary microflora is the second and we have compared these components with def index in children under 3-6 years of age group.[8]
In humans, early in fetal development is the time when dermal ridge differentiation takes place. By the 7th week of intrauterine life, development of primary palate and lip is completed and that of secondary palate is completed by 12th week of gestation.[9] The dermal ridges develop in relation to volar pads, which are formed by the 6th week of intrauterine life and it reaches maximum size between 12-13th week of gestation. Moreover, enamel is a structure of ectodermal origin same as that of palate and alveolar ridges and is most susceptible to caries. This proves that genetic messages contained in the genome, normal or abnormal, are deciphered during this period and reflected by dermatoglyphics.[10], [11], [12]
In this study, we have selected children between 3-6 years of age because, by this age window of infectivity would have been attained and complete set of deciduous dentition must have erupted so that S. mutans levels can be measured properly.[13] Incipient lesions of enamel transform into cavitation by 2-5 years of age; so, by this time any developed lesion would have started progressing and adding up to number of carious teeth. At this age group it can be well assured that it is the genetic susceptibility that determines cariogenic potential of enamel and as the age advances other factors also becomes much more significant in causation of dental caries. This theory justifies the rationale for selection of age group for this study.[14], [15], [16]
Early detection of dental caries can aid in initiation of preventive oral health measures at a very young age. Dermatoglyphics can prove to be a useful and cost-effective tool for preliminary investigations into conditions with a suspected genetic base.[17] There is a definite correlation between dermatoglyphics and dental caries presentation and bacterial count. In our study it was found that the increased frequency of the whorls in children is directly associated with higher def index and increased S. mutans count and vice-versa. On the other hand increased loop frequency is directly correlated with lower def index and decreased s. Multan count and vice-versa.
Conclusion
Dermatoglyphics pattern being a genetic marker for dental caries, are important and significant factor in the preliminary diagnosis of dental caries and other diseases with a genetic cause. This study supports and suggests use of dermatoglyphics as a strong diagnostic tool for caries detection at an early age which can help in prevention of caries occurrence in children. However, further research in the field of dermatoglyphics should be carried out for better understanding of the same in the field of dentistry and medicine.
Source of Funding
None.
Conflict of Interest
None.
References
- A Sharma, Somani. Dermatoglyphic Interpretation of Dental Caries and Its Correlation to Salivary Bacteria Interactions: An in-vivo Study. J Indian Soc Pedodon Prevent Dent 2009. [Google Scholar]
- AB Sengupta, BA Bazmi, S Sarkar, S Kar, C Ghosh, H Mubtasum. A Cross Sectional Study of Dermatoglyphics and Dental Caries in Bengalee Children. J Indian Soc Pedodontics Prevent Dent 2013. [Google Scholar]
- RPR Abhilash, Divyashree, MG Gouda Patil, T Gupta, Chandrasekar. Dermatoglyphics in Patients with Dental Caries: A Study on 1250 Individual.. J Contemp Dent Pract 2012. [Google Scholar]
- N Nemmarugommula, A Arun, H Mythri. Caries Activity Tests. Research and Reviews: . J Dent Sci 2013. [Google Scholar]
- VK Gopinath, AR Arzreanne. Saliva as a diagnostic tool for assessment of Dental caries. Arch Oro Sci 2006. [Google Scholar]
- T Sandhya, T Avinash, E Satheesan. Caries Activity Indicators: Guide for Dental Practitioners. Int J Oral Maxillofac Pathol 2012. [Google Scholar]
- DW Tamgire, RR Fulzele, VVK Chimurkar, SS Rawlani, AR Shekre. Quantitative Dermatoglyphics Analysis of Finger Tip Patterns of Oral Sub Mucous Fibrosis. J Dent Med Sci 2013. [Google Scholar]
- L Mathew, AM Hegde. Rai K Dermatoglyphic findings in oral clefts. J Indian Soc Pedod Prev Dent 2005. [Google Scholar]
- SB Holt. The hypothenar radial arch-A genetically determined epidermal ridge configuration. Am J Phy Anthrop 1975. [Google Scholar]
- JA Uchida, HC Solton. Evaluation of Dermatoglyphics in medical genetics. Pediatr Clin North Am 1963. [Google Scholar]
- EV Glanville. Heredity and line of palmar dermatoglyphics. Am J Hum Genet 1965. [Google Scholar]
- SK Hegde. Estimation of salivary capable of inhibiting and stimulating streptococcus mutans, and its correlation to dental caries and untreated carious teeth. J Indian Soc Pedod Prev Dent 2005. [Google Scholar]
- CV Pereira, LJ Pereira. In vitro bacterial plaque suppuration and recolonization by S.mutans and S.sobrinus. Braz J Microbiol 2006. [Google Scholar]
- BS Bolgül, S Celenk, BE Ayna, F Atakul, E Uysal. Evaluation of caries risk factors and effects of a fluoride-releasing adhesive material in children with insulin-dependent diabetes mellitus (IDDM): Initial first-year results. Acta Odontol Scand 2004. [Google Scholar]
- GK Stookey. Effect of saliva on dental caries. J Am Dent Assoc 2008. [Google Scholar]
- R J Gibbons, J V Houte. Bacterial adherence in oral microbial ecology. A Rev Microbiol 1975. [Google Scholar]
- M Atasu. Dermatoglyphic findings in Dental caries: A preliminary report. J Clin Pediatr Dent Winter 1998. [Google Scholar]